Therapeutic Uses of Rituximab in Pediatrics
Rituximab Therapy in Pediatrics
Chief Mentor: Dr. A. Narendra (Assistant Professor, Pediatrics)
Biologic Advancements: Targeted B-Cell Depletion
"Residents and interns, Rituximab has transformed the management of refractory pediatric autoimmune and renal conditions. Master its chimeric molecular structure, distinct mechanisms of cell death, and clinical indications for your theory papers and clinical grand rounds."
— Dr. A. Narendra
High-Yield Examination Blueprints
Molecular Identification: Rituximab is a genetically engineered chimeric mouse/human monoclonal antibody (IgG1 kappa) targeted explicitly against the CD20 antigen found on the surface of B-lymphocytes.
B-Cell Lifespan Targeting Specificity:
- Expressed prominently on: Pre-B cells, mature B cells, and memory B cells.
- Crucial Exam Fact: It spares hematopoietic stem cells and mature **plasma cells** (as plasma cells lose the CD20 marker). Hence, baseline immunoglobulin production is partially preserved.
Three Triad Mechanisms of B-Cell Lysis:
- Complement-Dependent Cytotoxicity (CDC): Rituximab binding triggers the classical complement pathway, generating the membrane attack complex ($MAC$) to punch holes in the B-cell membrane.
- Antibody-Dependent Cellular Cytotoxicity (ADCC): Natural Killer ($NK$) cells and macrophages recognize the Fc portion of Rituximab, releasing perforins and granzymes to lyse the B cell.
- Direct Induction of Apoptosis: Cross-linking of CD20 directly activates intracellular caspase pathways, accelerating programmed cell death.
1. Steroid-Dependent Nephrotic Syndrome (SDNS) & Frequently Relapsing NS (FRNS)
Rituximab serves as a highly effective steroid-sparing agent. It helps maintain long-term remission, breaks the cycle of frequent relapses, and allows for the safe taper of toxic corticosteroids and calcineurin inhibitors.
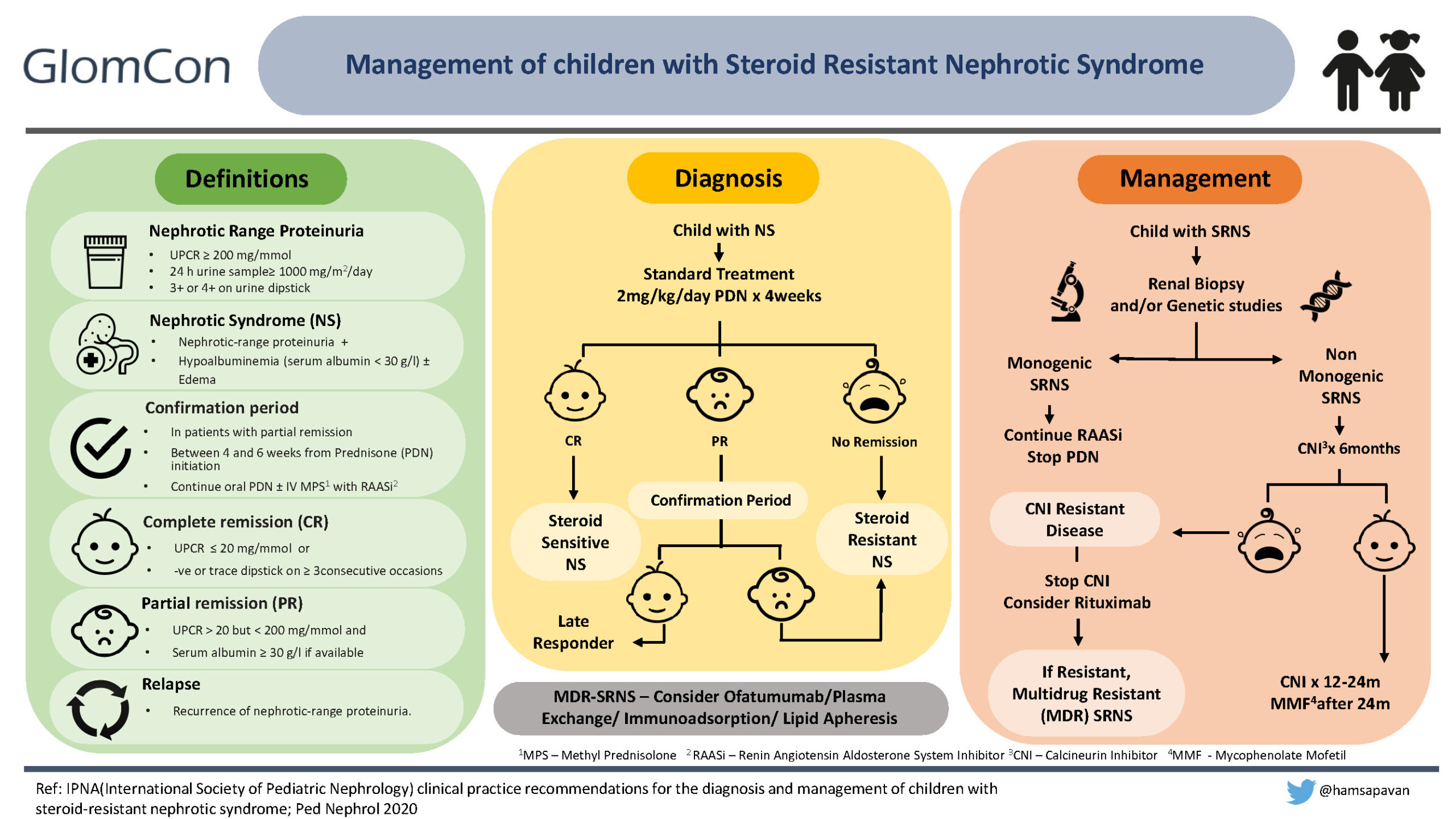
2. Refractory Steroid-Resistant Nephrotic Syndrome (SRNS)
In children with non-genetic forms of SRNS who fail to achieve remission with Cyclosporine or Tacrolimus, Rituximab can be utilized to reduce proteinuria and protect long-term GFR.
3. Lupus Nephritis (Class III, IV, or V)
Indicated in severe, active pediatric lupus nephritis that shows an inadequate response to standard induction therapy with Mycophenolate Mofetil (MMF) or Cyclophosphamide.
Rheumatology Systemic Disease Indications:
- ANCA-Associated Vasculitis: Granulomatosis with Polyangiitis (GPA / Wegener's) and Microscopic Polyangiitis (MPA). Rituximab is FDA-approved for induction therapy here, matching Cyclophosphamide efficacy with less gonadal toxicity.
- Severe Juvenile Dermatomyositis (JDM): Indicated in refractory JDM presenting with severe skin ulcerations or progressive proximal muscle weakness unresponsive to high-dose pulse steroids and Methotrexate.
Hematology Indications (Antibody-Mediated Destruction):
- Refractory Immune Thrombocytopenia (ITP): Used in chronic or severe ITP with high bleeding risk that fails to respond to IVIg, Anti-D, or corticosteroids.
- Autoimmune Hemolytic Anemia (AIHA): Highly effective in severe warm or cold-antibody AIHA and **Evans Syndrome** (co-existing ITP and AIHA).
Dosing Protocols: Typically administered as **$375 \text{ mg/m}^2$ IV infusion** once weekly for 2 to 4 doses, or alternative rheumatology regimens ($750 \text{ mg/m}^2$ two doses, 2 weeks apart).
Adverse Reactions Checklist
- Acute Infusion Reactions: Fever, chills, bronchospasm, and hypotension (caused by massive cytokine release).
- Severe Cytopenias: Late-onset neutropenia can occur months post-therapy.
- Hypogammaglobulinemia: Prolonged B-cell depletion leads to low IgG levels, increasing the risk of sinopulmonary infections.
- PML Risk: Progressive Multifocal Leukoencephalopathy (rare JC virus reactivation).
Dr. Narendra's Screening Protocol
- Pre-medication Mandate: Always give Paracetamol, Pheniramine/Diphenhydramine, and Hydrocortisone 30 minutes before starting the infusion.
- Viral Screening: Screen for Hepatitis B (HBsAg and Anti-HBc) before the first dose to prevent fatal reactivation.
- Immunization Rule: Complete all required live vaccines at least 4 weeks before starting therapy. Live vaccines are contraindicated during B-cell depletion.


Quiz Performance Tracker
Updates instantly as you click 'Verify Answer' in the MCQs tab.
Pre-Infusion Checklist
- Complete HBV Serology Screening
- Document baseline IgG, IgA, IgM levels
- Verify CBC with absolute neutrophil count
- Confirm no live vaccines were given in past 4 wks
Dr. Narendra's PG Pearls
"When writing your answers on Steroid-Dependent Nephrotic Syndrome, make sure to highlight the **CD20 B-cell depletion remission axis**. Rituximab doesn't just clear standard autoantibodies; it also helps stabilize the podocyte actin cytoskeleton directly by preventing the downregulation of sphingomyelin phosphodiesterase acid-like 3b (SMPDL-3b) during severe systemic exposures."

Comments
Post a Comment